Abstract
The Islamic Republic of Iran's health system is divided into three levels: the first level is the Primary Health Care (PHC) system, the second level includes specialized polyclinics/clinics, general and specialized hospitals, and the third level is the sub-specialized hospitals. Based on the available evidence, Iran's HS has evolved and progressed since 1984, becoming a comprehensive, public-centered, responsive, and cost-effective system, (Figure 1) (1,2).

During the COVID-19 pandemic, countries reacted differently based on their HS infrastructure and structure, available primary resources (financial and human resources), and the severity of the disease spread. Evidence reveals that most countries relied on their hospitals and health systems to combat the COVID-19 epidemic. However, the health system’s response was slightly different in the Islamic Republic of Iran. Since the early days of identifying cases and preparing hospitals for admission and treatment of COVID-19 patients, the PHC system initiated a comprehensive reaction to combat the COVID-19 pandemic as the first line and the first point of the HS's contact with the community. In this regard, the PHC system determined the principal policies for combating COVID-19 as follows (3):
- General vaccination based on the priorities in the national document Provision of active and essential healthcare and services (in-person/remotely)
- Early identification of COVID-19 cases and tracing their close contacts (family/workplace)
- Protection and isolation of vulnerable populations (reverse quarantine
- Ensuring compliance with isolation and quarantine rules (hotel quarantine and house quarantine)
- Development and improvement of outpatient COVID-19 treatment
Different solutions and strategies have been devised to implement and fulfill the determined policies, which can be divided into three general categories:
a) Modifying the structure of service delivery
b) Modifying the programs and procedures
c) Improving the methods of service provision
Strategy 1: The first strategy is to make structural changes in the PHC system (Figure 2), which occurred in the first week of the outbreak in the Iran’s PHC system. Through alterations in structure, human resources, duties, and function, 1200 comprehensive urban (1099) and rural (111) health centers were designated as COVID -19 centers for suspected COVID-19 outpatients from rural health houses, urban health posts, rural/urban comprehensive health service centers, and other private centers.

These centers have several primary functions: initial triage, diagnosis, primary care, physician visit, medical treatment based on the national outpatient treatment protocol, and conducting diagnostic COVID-19 tests.The second structural change is the development of COVID-19 diagnostic laboratories and the setting up of a rationalized laboratory system in PHC. Before the COVID-19 pandemic, only two laboratories could detect COVID-19 in the PHC system, which has since been increased to 129 well-equipped and active laboratories in the public sector and 304 laboratories in the private and nongovernmental sectors (433 laboratories). The third change was extensive modifications to the PHC system to develop permanent testing units in selected COVID-19 centers and mobile testing units in the vicinity of individuals’ homes and workplaces (4,5).The fourth structural change is establishing the Health Observatory Center to analyze and aggregate data related to the COVID-19 pandemic and vaccination, evaluate the situation by city and province, and report for evidence-based policy. A multidisciplinary team of specialists in IT, epidemiology, statistics and vital health indicators, and communicable disease management is responsible for the abovementioned tasks (6).The fifth structural change is the establishment of COVID-19 mass vaccination centers. In order to prevent any disruption in regular essential health services, vaccination posts and specialized centers were constructed in cities with a population of over 20,000 to provide care services for infants, children, adolescents, young people, pregnant mothers, middle-aged and the elderly. According to the national COVID-19 vaccination document,1,228 vaccination posts with more than 6,490 stations were set up across the country to deliver vaccinations based on the registration of age groups. The vaccinations were administered by the PHC system staff (health workers and HC providers), volunteer organizations such as Basij Organization, the General Staff of the Armed Forces, the Red Crescent, and other organizations with the broad participation of community health volunteers (neighborhood health liaisons and family health ambassadors), and university students.
Strategy 2: The second anticipated strategy is a modification in the content and program of the PHC system. Iran is one of the first countries to design an outpatient treatment protocol at the first level of care for COVID-19 (7), which has been reviewed, revised, and updated nine times according to the latest scientific findings and national experiences (8).The second major shift in the PHC system occurred three months following the outbreak, and involved a review of all healthcare and service packages for all age groups. Within two months, all service packages were reviewed by specialized teams and divided into two parts: in-person care and services (services that are provided in-person), and remote services and care (services that can be provided remotely and do not require in-person visits), which could help people avoid unnecessary HC unit visits, thus avoiding congestion, traffic, and possible outbreaks (9).The third change is to provide COVID-19 service and care package for refugees and foreign nationalities, pregnant mothers, children under five, nomadic communities, prisoners, people with chronic diseases, and the elderly. The HS considered mentioned groups vulnerable who required special attention; therefore, a unique action plan was developed and published for constant control and proper care (10,11).The fourth change is the development of COVID-19 health protocols for specific occupations in different classes and professions. Within a month, 165 protocols were developed for 24,000 high-risk jobs (12).
Strategy 3: Changes in the methods of service provision is the third primary strategy; the first change in methods was telephone counseling applying the telephone numbers 4030, 190, and 1666 (health insurance) (Figure 3). These hotlines are for counseling, educating, and referring suspicious, probable, and confirmed cases according to a COVID-19 system.
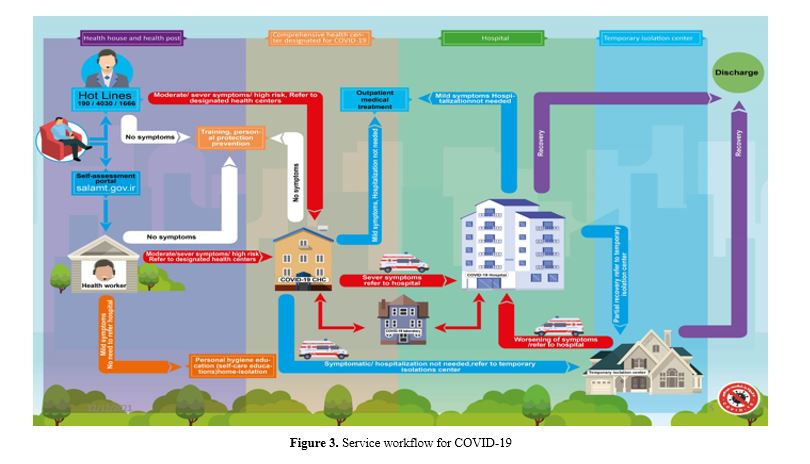
The second method is designing the salamat.gov.ir website for direct virtual communication with people to manage and control the COVID-19 pandemic. This system exhibited different functions in different stages of pandemic management. The system’s capabilities are educational functions, screening, referral, occupation registration, vaccination enrollment, and scheduling of COVID-19 vaccination.The salamat.gov.ir website has been used for the COVID-19 self-assessment and referral since the inception of the COVID-19 outbreak. The whole process is based on HS’s framework. People assessed their health status by visiting the site and reviewing the signs and symptoms of COVID-19. Then, necessary education and recommendations for prevention and care were provided based on the assessment result by health workers (Behvarz and Morageb-e-Salamat). In addition, a text message containing guidelines and educational tips was sent to individuals. Eventually, based on the self-assessment results and the disease status, the health workers (HWs) or the relevant HC providers would provide essential training and guidance for staying at home and instructions for urgent conditions via phone. In some cases, based on the deterioration of the patients’ conditions, they would be referred to the selected COVID-19 centers or the designated COVID-19 hospitals (13).The third method is the verbal screening of the population covered by HWs in rural and urban areas. HWs made phone calls to the families in their service area to find out if any members of the family experienced any COVID-19-related symptoms. Thereby, if anyone were infected, HWs would perform based on the approach in Figure 3 (13).The fourth method of the third strategy is to register occupations and industries in the salamat.gov.ir website for screening, training, and reopening according to the color-coding of cities based on the prevalence of COVID-19 cases, hospitalization, and mortality rates. The mentioned method is performed constantly and provides an online opportunity for public monitoring based on the specific QR code. In this regard, more than 2,300,000 jobs were registered and received a unique tracking and monitoring code (QR code).The fifth method included diagnosis, care, tracing, testing, and neighborhood-based monitoring according to the HC system. The geographical area covered by health houses and rural comprehensive health centers, health posts, and urban comprehensive health centers in all cities provides the basis for classification, intervention, and early detection of suspected, probable, and confirmed COVID-19 cases and their close contacts. In addition, they provide isolation, care, and quick treatment for patients with COVID-19 (14).Four operational teams were used to implement these interventions: 1- contact tracing teams, 2- home care teams, 3- supervisory teams, and 4- support teams. All teams, using the neighborhood-based model, carried out the designated tasks with the help of the Basij Organization, the Red Crescent, NGOs, and other volunteer organizations.The sixth method is aggregating information and establishing a Corona Hub at the Health Observatory Center (Figure 4). All the data related to COVID-19 in the service delivery facilities have been aggregated through electronic health record systems, Mask application, and web services, and then displayed in specific management dashboards.
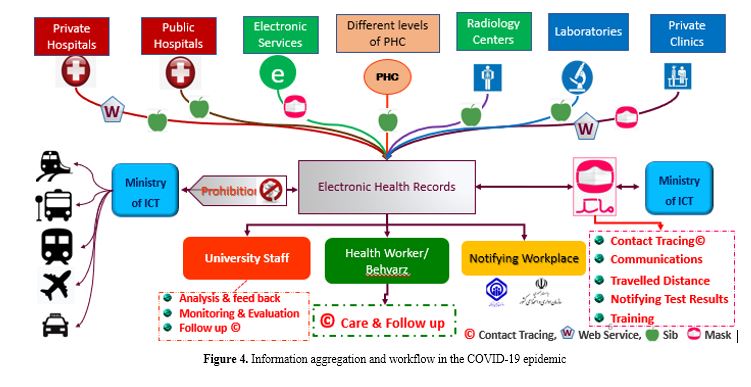
The information from Corona Hub were used to apply different types of restrictions and reopening policies. It also provided general education about social distancing, identification, screening, and care of patients and close contacts. Informing employers and declaring compensation payments also happened through Corona Hub (on behalf of welfare and Social Security Organization) (3).The seventh method is the mass vaccination of COVID-19, based on the national vaccination document and the PHC system. Vaccination is performed in rural areas, mainly by Health Houses and Comprehensive Health Centers. Daily COVID-19 vaccinations are administered in the attached health houses, under a physician's supervision. Also, in other health houses, vaccinations are performed according to the physician's visit schedule and invitation by the HWs based on the booking system. In cities with fewer than 20,000 inhabitants, health posts provide vaccinations under a physician's supervision. However, in towns with more than 20,000 inhabitants, mass vaccinations are administered by health posts (3,15).